Introduction
This document details the methodology for the Lower Gastrointestinal Hemorrhage measure and should be reviewed along with the Lower Gastrointestinal Hemorrhage Measure Codes List file, which contains the medical codes used in constructing the measure.
Measure Description
Episode-based cost measures represent the cost to Medicare for the items and services provided to a patient during an episode of care (“episode”). In all supplemental documentation, “cost” generally means the standardized Medicare allowed amount, and claims data from Medicare Parts A and B are used to construct the episode-based cost measures.
The Lower Gastrointestinal Hemorrhage episode-based cost measure evaluates a clinician’s risk-adjusted cost to Medicare for beneficiaries who receive inpatient non-surgical treatment for acute bleeding in the lower gastrointestinal tract during the performance period. The cost measure score is the clinician’s risk-adjusted cost for the episode group averaged across all episodes attributed to the clinician. This acute inpatient medical condition measure includes costs of services that are clinically related to the attributed clinician’s role in managing care during each episode from the clinical event that opens, or “triggers,” the episode through 35 days after the trigger.
Measure Rationale
Gastrointestinal bleeding is the most common cause of hospitalizations among gastrointestinal diseases, with over 500,000 patients hospitalized annually. Lower gastrointestinal bleeding is responsible for approximately 30 to 40 percent of all gastrointestinal bleeding cases, with an incidence of around 36 per 100,000 persons. Morbidity and mortality due to GI bleeds increase significantly for patients who are older and for those with pre-existing medical conditions, leading to higher costs and resource use, including for Medicare patients. With application of an effective measurement tool, opportunities for improvement in care of lower gastrointestinal bleeding include better methods for characterizing patients at higher risk for re-bleeding, better approaches to treatment and ongoing management to reduce the incidence of recurrent bleeding, and improving the use of early intervention strategies to mitigate the risk for catastrophic bleeding and other associated downstream complications. The Lower Gastrointestinal Hemorrhage episode-based cost measure was recommended for development by an expert clinician committee—the Gastrointestinal Disease Management – Medical and Surgical Clinical Subcommittee—because of its high impact in terms of patient population and Medicare spending, and the opportunity for incentivizing cost-effective, high-quality clinical care in this area. Based on the initial recommendations from the Clinical Subcommittee, the subsequent measure-specific workgroup provided extensive, detailed input on this measure.
Measure Numerator:
The cost measure numerator is the sum of the ratio of observed to expected payment-standardized cost to Medicare for all Lower Gastrointestinal Hemorrhage episodes attributed to a clinician. This sum is then multiplied by the national average observed episode cost to generate a dollar figure.
Measure Denominator:
The cost measure denominator is the total number of episodes from the Lower Gastrointestinal Hemorrhage episode group attributed to a clinician.
Data Sources
The Lower Gastrointestinal Hemorrhage cost measure uses the following data sources:
- Medicare Parts A and B claims data from the Common Working File (CWF)
- Enrollment Data Base (EDB)
- Long Term Care Minimum Data Set (LTC MDS)
Care Settings
Methodologically, the Lower Gastrointestinal Hemorrhage cost measure can be triggered based on claims data from the following settings: acute inpatient (IP) hospitals.
Cohort
The cohort for this cost measure consists of patients who are Medicare beneficiaries enrolled in Medicare fee-for-service and who receive inpatient non-surgical treatment for acute bleeding in the lower gastrointestinal tract that triggers a Lower Gastrointestinal Hemorrhage episode.
The cohort for this cost measure is also further refined by the definition of the episode group and measure-specific exclusions (see Appendix A).
Methodology Steps
There are two overarching processes in calculating episode-based cost measure scores: episode construction (Steps 1-3) and measure calculation (Steps 4-6). This section provides a brief one-page summary of these processes for the Lower Gastrointestinal Hemorrhage cost measure, and Appendix A describes the processes in detail.
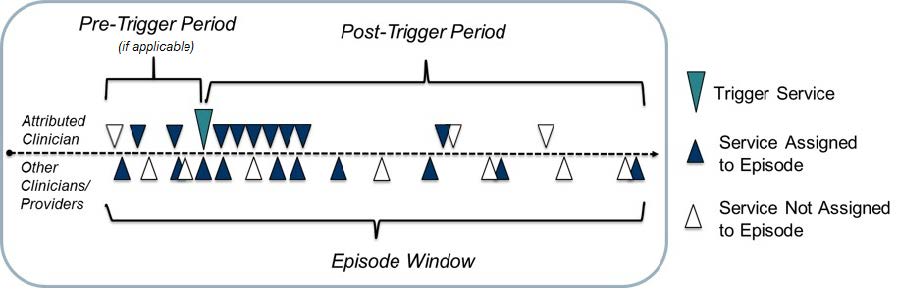
- Trigger and define an episode: Episodes are defined by billing codes that open, or “trigger,” an episode. The episode window starts 90 days before the trigger and ends 30 days after the trigger. To enable meaningful clinical comparisons, episodes are placed into more granular, mutually exclusive sub-groups based on clinical criteria. Some episodes may also be excluded based on other information available at the time of the trigger.
- Attribute the episode to a clinician: For this procedural episode group, an attributed clinician is any clinician who bills a trigger code for the episode group on the day of the procedure for outpatient procedures or during the inpatient stay for inpatient procedures.
- Assign costs to the episode and calculate the episode observed cost: Clinically related services occurring during the episode window are assigned to the episode. The cost of the assigned services is summed to determine each episode’s standardized observed cost.

- Exclude episodes: Exclusions remove unique groups of patients from cost measure calculation in cases where it may be impractical and unfair to compare the costs of caring for these patients to the costs of caring for the cohort at large.
- Calculate expected costs for risk adjustment: Risk adjustment aims to isolate variation in clinician costs to only the costs that clinicians can reasonably influence (e.g., accounting for beneficiary age, comorbidities and other factors). A regression analysis is run using the risk adjustment variables as covariates to estimate the expected cost of each episode. Then, statistical techniques are applied to reduce the effect of extreme outliers on measure scores.
- Calculate the measure score: For each episode, the ratio of standardized total observed cost (from step 3) to risk-adjusted expected cost (from step 5) is calculated and averaged across all of a clinician or clinician group’s attributed episodes to obtain the average episode cost ratio. The average episode cost ratio is multiplied by the national average observed episode cost to generate a dollar figure for the cost measure score.
Measure Specifications Quick Reference
This page provides a quick, at-a-glance reference for the Lower Gastrointestinal Hemorrhage episode-based cost measure specifications. More details on each component can be found in Appendix A, and the full list of codes and logic used to define each component can be found within the Measure Codes List file.
| Episode Window: During what time period are costs measured? | |
| Pre-Trigger Window: 0 days | Post-Trigger Window: 35 days |
| Triggers: Patients receiving what medical care are included in the measure? | |
| |
| Service Assignment: Which clinically related costs are included in the measure? | |
Assigned services generally fall within the following clinical themes:
| |
| Risk Adjustors: Which risk factors are accounted for in the risk adjustment model? | Exclusions: Which populations are excluded from measure calculation? |
|
|
Appendix A. Detailed Measure Methodology
This section contains the technical details for the two overarching processes in calculating episode-based cost measure scores in more detail: Sections A.1 through A.3 describe episode construction and Sections A.4 through A.6 describe measure calculation.
Trigger and Define an Episode
Lower Gastrointestinal Hemorrhage episodes are defined by Medicare Severity Diagnosis-Related Group (MS-DRG) codes that open, or trigger, an episode. Specifically, episodes are triggered by the occurrence of IP E&M codes on Part B Physician/Supplier claims during an IP facility stay with a specified MS-DRG. For the codes and logic relevant to this section please see the “Triggers” and “Triggers_Details” tabs of the Lower Gastrointestinal Hemorrhage Measure Codes List.
The steps for defining an episode for the Lower Gastrointestinal Hemorrhage episode group are as follows:
- Identify Part B Physician/Supplier claim lines with positive standardized payment that have a trigger code.
- Trigger an episode if all the following conditions are met for an identified Part B Physician/Supplier claim line:
- It was billed by a clinician of a specialty that is eligible for MIPS.
- It does not have a post-operative modifier code.
- It is the highest cost claim line across all claim lines identified in the above bullets and that have any Renal or Ureteral Stone Surgical Treatment trigger code billed for the beneficiary on that day. If multiple Part B Physician/Supplier claim lines with a trigger code occur on different days within a concurrent IP stay, an episode will be triggered by the claim line with the earliest expense date during the IP stay.
- Identify episodes that have a concurrent IP stay by identifying the first IP stay with a relevant Medicare Severity Diagnosis-Related Group (MS-DRG) code for the beneficiary that is concurrent to the expense date for the trigger Part B Physician/Supplier claim line.
- Establish the episode window as follows:
- Establish the episode trigger date as the date of admission if an IP stay with a relevant DRG concurrent with the trigger is found, otherwise the expense date of the trigger code.
- Establish the episode start date as 90 days prior to the episode trigger date.
- Establish the episode end date as 30 days after the episode trigger date.
Attribute Episodes to a Clinician
Once an episode has been triggered and defined, it is attributed to one or more clinicians of a specialty that is eligible for MIPS. Clinicians are identified by Taxpayer Identification Number (TIN) and National Provider Identifier (NPI) pairs (TIN-NPI), and clinician groups are identified by TIN. Only clinicians of a specialty that is eligible for MIPS or clinician groups where the triggering clinician is of a specialty that is eligible for MIPS are attributed episodes. For an example of how attribution works for acute inpatient medical condition episodes, please refer to Appendix B. For codes relevant to this section, please see the “Attribution” tab of the Lower Gastrointestinal Hemorrhage Measure Codes List.
The steps for attributing a Lower Gastrointestinal Hemorrhage episode are as follows:
- Identify Part B Physician/Supplier claim lines for which all of the following conditions are true:
- They have an expense date concurrent to the trigger IP stay.
- They have a CPT/HCPCS code included in the list of IP E&M codes for TIN-NPI attribution.
- Attribute an episode to a TIN if that TIN billed at least 30 percent of the IP E&M codes on identified Part B Physician/Supplier claim lines during the trigger IP stay.
- Attribute the episode to a TIN-NPI if a clinician within an attributed TIN billed any IP E&M codes on identified Part B Physician/Supplier claim lines during the IP stay.
Future attribution rules may benefit from the implementation of patient relationship categories and codes. As required by section 101(f) of MACRA, CMS will consider how to incorporate the patient relationship categories into episode-based cost measurement methodology as clinicians and billing experts gain experience with them.
Assign Costs to an Episode and Calculate Total Observed Episode Cost
Services, and their Medicare costs, are assigned to an episode only when clinically related to the attributed clinician’s role in managing patient care during the episode. Assigned services may include treatment and diagnostic services, ancillary items, services directly related to treatment, and those furnished as a consequence of care (e.g., complications, readmissions, unplanned care, and emergency department visits). Unrelated services are not assigned to the episode. For example, the cost of care for a chronic condition that occurs during the episode but is not related to the clinical management of the patient relative to the acute lower gastrointestinal tract bleeding would not be assigned.
To ensure that only clinically related services are included, services during the episode window are assigned to the episode based on a series of service assignment rules, which are listed in the “Service_Assignment” tab of the Lower Gastrointestinal Hemorrhage Measure Codes List file.
For the Lower Gastrointestinal Hemorrhage episode group, only services performed in the following service categories are considered for assignment to the episode costs:
- Emergency Department (ED)
- Outpatient (OP) Facility and Clinician Services
- IP – Medical
- IP – Surgical
- Inpatient Rehabilitation Facility (IRF) – Medical
- Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DME)
- Home Health (HH)
In addition to service category, service assignment rules may be modified based on the service category in which the service is performed, as listed above. Service assignment rules may also be defined based on specific (i) service information alone or service information combined with diagnosis information, (ii) prior incidence of service, and/or (iii) the timing of the service, as detailed below.
- Services may be assigned to the episode based on the following service information combinations:
- High level service code alone
- High level service code combined with first three digits of the International Classification of Diseases – Tenth Revision diagnosis code (3-digit ICD-10 diagnosis code)
- High level service code combined with full ICD-10 diagnosis code
- High level service code combined with more specific service code
- High level service code combined with more specific service code and with 3-digit ICD-10 diagnosis code
- High level service code combined with more specific service code and with full ICD-10 diagnosis code
- Assigned services may be further refined by prior incidence of service or diagnosis:
- Services may be assigned unconditionally (regardless of prior incidence of the service in patient’s recent claims history)
- Services may be assigned if newly occurring
- Services may be assigned in combination with a diagnosis if the service is newly occurring
- Services may be assigned in combination with a diagnosis if the diagnosis is newly occurring
- Services may be assigned in combination with a diagnosis if either the service OR the diagnosis are newly occurring
- Services may be assigned in combination with a diagnosis if both the service AND the diagnosis are newly occurring
- Services as defined by the applicable combinations and incidence options above may be assigned with only specific timing:
- Services may be assigned based on whether or not the service occurs before the trigger (in the pre-trigger window) and/or after the trigger (in the post-trigger window)
- Services may be assigned only if they occur within a particular number of days from the trigger within the episode window, and services may be assigned for a period shorter than the full duration of the episode window
The steps for assigning costs are as follows:
- Identify all services on claims with positive standardized payment that occur within the episode window.
- Assign identified services to the episode based on the types of service assignment rules described above.
- Assign skilled nursing facility (SNF) claims based on the following criteria:
- Identify SNF claims for which both (i) the SNF claim’s qualifying IP stay is the IP stay during which the trigger occurs, if an IP stay is found, and (ii) the SNF claim occurs during the episode window.
- For those identified SNF claims, assign the percentage of the claim amount proportional to the portion of the SNF claim that overlaps with the episode window.
- Assign all claims with trigger codes occurring during the trigger day/stay.
- Assign all physician claims and DME claims occurring during concurrent IP stay.
- Assign all inpatient E&M claims during IP stays in the post-trigger window assigned to episode.
- Sum standardized Medicare allowed amounts for all claims assigned to each episode to obtain the standardized total observed episode cost.
Service Assignment Example
- Clinician A performs surgical treatment for renal or ureteral stones for Patient K. This service triggers a Renal or Ureteral Stone Surgical Treatment episode, which is attributed to Clinician A.
- Clinician B treats the patient for post-operative urinary tract infection (UTI), which is considered a clinically related service, during the episode window.
- Because post-operative treatment for UTI during the episode window is considered to be clinically related to the initial surgical treatment for renal or ureteral stones, the cost of the post-operative treatment for UTI will be assigned to Clinician A’s Renal or Ureteral Stone Surgical Treatment episode.
Exclude Episodes
Before measure calculation, episode exclusions are applied to remove certain episodes from measure score calculation. Certain exclusions are applied across all acute inpatient medical condition episode groups, and other exclusions are specific to this measure, based on consideration of the clinical characteristics of a homogenous patient cohort. The measure-specific exclusions are listed in the “Exclusions” and “Exclusions_Details” tabs in the Lower Gastrointestinal Hemorrhage Measure Codes List file.
The steps for episode exclusion are as follows:
- Exclude episodes from measure calculation if:
- The beneficiary has a primary payer other than Medicare for any time overlapping the episode window or 120-day lookback period prior to the trigger day.
- The beneficiary was not enrolled in Medicare Parts A and B for the entirety of the lookback period plus episode window, or was enrolled in Part C for any part of the lookback plus episode window.
- No main clinician is attributed the episode.
- The beneficiary’s date of birth is missing.
- The beneficiary’s death date occurred before the episode ended.
- The episode trigger claim was not performed in an ambulatory/office-based care, IP hospital, OP hospital, or ASC setting based on its place of service.
- The IP facility is not a short-term stay acute hospital as defined by subsection (d) when an IP stay concurrent with the trigger is found.
- Apply measure-specific exclusions, which check the beneficiary’s Medicare claims history for certain billing codes (as specified in the Measure Codes List file) that indicate the presence of a particular procedure, condition, or characteristic.
Estimate Expected Costs through Risk Adjustment
Risk adjustment is used to estimate expected episode costs in recognition of the different levels of care beneficiaries may require due to comorbidities, disability, age, and other risk factors. The risk adjustment model includes variables from the CMS Hierarchical Condition Category Version 22 (CMS-HCC V22) 2016 Risk Adjustment Model, as well as other standard risk adjustors (e.g., beneficiary age) and variables for clinical factors that may be outside the attributed clinician’s reasonable influence. A full list of risk adjustment variables can be found in the “RA” and “RA_Details” tabs of the Lower Gastrointestinal Hemorrhage Measure Codes List file.
Steps for defining risk adjustment variables and estimating the risk adjustment model are as follows:
- Define HCC and episode group-specific risk adjustors using service and diagnosis information found on the beneficiary’s Medicare claims history in the 120-day period prior to the episode trigger day (or the timing specified in the “RA_Details” tab of the Measure Codes List file) for certain billing codes that indicate the presence of a procedure, condition, or characteristic.
- Define other risk adjustors that rely upon Medicare beneficiary enrollment and assessment data as follows:
- Identify beneficiaries who are originally “Disabled without end-stage renal disease (ESRD)” or “Disabled with ESRD” using the original reason for joining Medicare field in the Medicare beneficiary enrollment database (EDB).
- Identify beneficiaries with ESRD if their enrollment indicates ESRD coverage, ESRD dialysis, or kidney transplant in the Medicare beneficiary enrollment database in the lookback period.
- Identify beneficiaries who have spent at least 90 days in a long-term care institution without having been discharged to the community for 14 days, based on MDS assessment data.
- Drop risk adjustors that are defined for less than 15 episodes nationally for each sub-group to avoid using very small samples.
- Categorize beneficiaries into age ranges using their date of birth information in the Medicare beneficiary enrollment database. If an age range has a cell count less than 15, collapse this in the next adjacent age range category towards the reference category (65-69).
- Include the MS-DRG of the episode’s trigger IP stay, if an IP stay is found, as a categorical risk adjustor.
- Run an ordinary least squares (OLS) regression model to estimate the relationship between all the risk adjustment variables and the dependent variable, the standardized observed episode cost, to obtain the risk-adjusted expected episode cost. A separate OLS regression is run for each episode sub-group nationally.
- Winsorize expected costs as follows.
- Assign the value of the 0.5th percentile to all expected episode costs below the 0.5th percentile.
- Renormalize values by multiplying each episode’s winsorized expected cost by the sub-group’s average expected cost, and dividing the resultant value by the sub-group’s average winsorized expected cost.
- Exclude episodes with outliers as follows. This step is performed separately for each sub-group.
- Calculate each episode’s residual as the difference between the re-normalized, winsorized expected cost computed above and the observed cost.
- Exclude episodes with residuals below the 1st percentile or above the 99th percentile of the residual distribution.
- Renormalize the resultant expected cost values by multiplying each episode’s winsorized expected costs after excluding outliers by the sub-group’s average standardized observed cost across all episodes originally in the risk adjustment model, and dividing by the sub-group’s average winsorized expected cost after
excluding outliers.
Calculate Measure Scores
Measure scores are calculated for a TIN or TIN-NPI as follows:
- Calculate the ratio of observed to expected episode cost for each episode attributed to the clinician/clinician group.
- Calculate the average ratio of observed to expected episode cost across the total number of episodes attributed to the clinician/clinician group.
- Multiply the average ratio of observed to expected episode cost by the national average observed episode cost to generate a dollar figure representing risk-adjusted average episode cost.
The clinician-level or clinician group practice-level risk-adjusted cost for any attributed clinician (or clinician group practice) “j” can be represented mathematically as:

where:
| ??? | is the standardized payment for episode i and attributed clinician (or clinician group practice) j |
| ? ?? | is the expected standardized payment for episode i and clinician (or clinician group practice) j, as predicted from risk adjustment |
| ?? | is the number of episodes for clinician (or clinician group practice) j |
| ? | is the total number of TIN/TIN-NPI attributed episodes nationally |
| is all episodes i in the set of episodes attributed to clinician (or clinician group practice) j |
A diagram demonstrating a visual depiction of an example measure calculation can be found in Appendix B.
Appendix B. Attribution Example for Acute Inpatient Medical Condition Episodes
This appendix provides some further details and an example of attribution for acute inpatient medical condition episodes. An episode is attributed to a:
- TIN if that TIN billed at least 30 percent of the IP E&M codes on identified Part B Physician/Supplier claim lines during the trigger IP stay, and to a
- TIN-NPI if a clinician within an attributed TIN billed any IP E&M codes on identified Part B Physician/Supplier claim lines during the trigger IP stay.
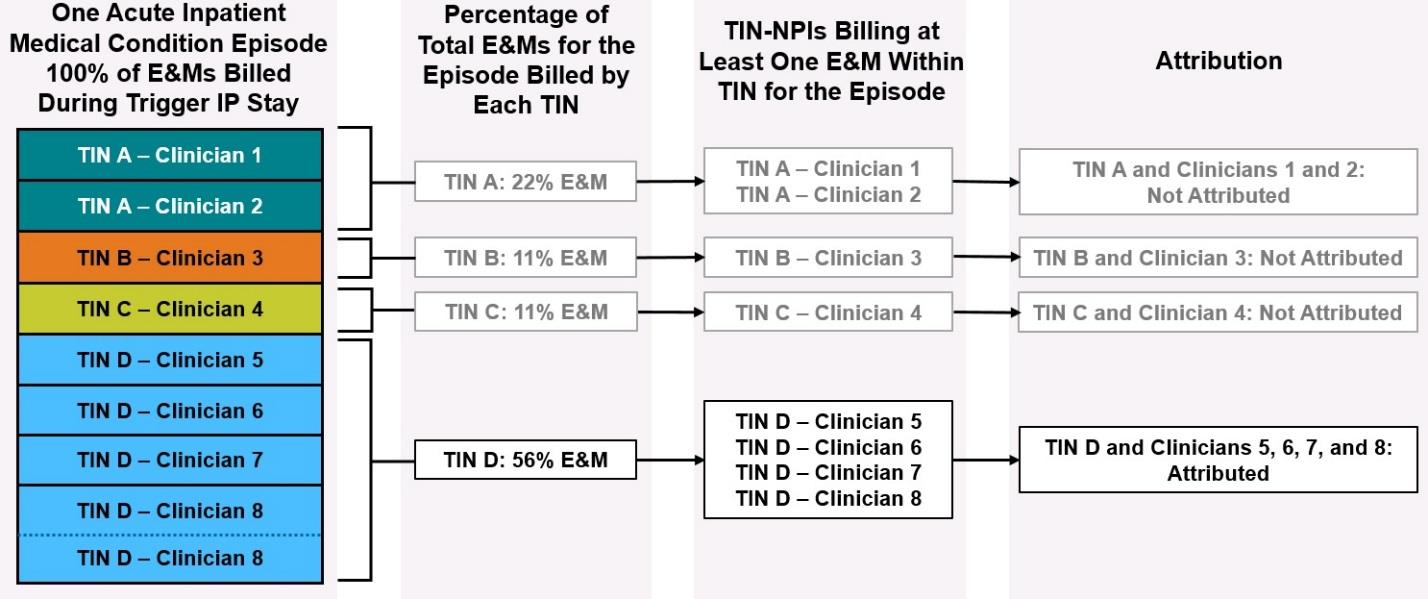
In the example shown above, the stacked, colored boxes on the left represent E&Ms billed by eight different TIN-NPIs (Clinicians 1 through 8) across four TINs (TINs A through D) in the trigger IP stay for one acute inpatient medical condition episode. Clinicians 1 through 7 each billed one E&M claim each under their respective TINs, and Clinician 8 billed two E&M claims under TIN D. The next set of boxes to the right of the colored boxes shows the percentage of total E&Ms for that trigger IP stay billed that were by each of the four TINs. Moving right, the next set of boxes list the clinicians within each of the four TINs who had billed at least one E&M during the trigger IP stay. Finally, the diagram shows a summary of how this affects attribution.
In this example, only TIN D billed at least 30 percent of the IP E&M codes